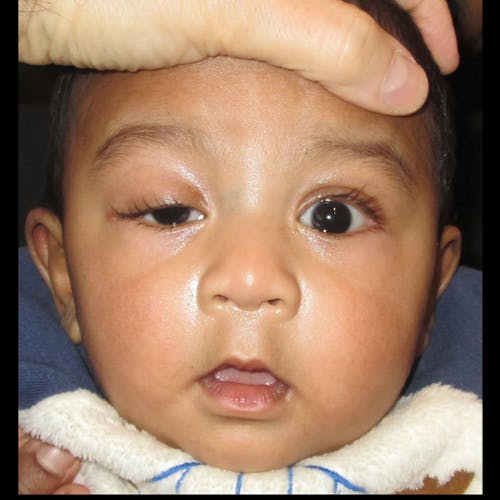
An infant or child with ptosis has a drooping upper eyelid that may interfere with vision. At The Pediatric Eye Center, we can correct this condition to restore normal eyelid function and support your child’s long-term visual development.


Understanding Congenital Ptosis
Congenital ptosis results from abnormal muscle and connective tissue development that lifts the eyelid. While it can be linked to certain syndromes, most cases occur on their own. A hallmark sign is that the affected lid does not lower completely when the eyes look down, known as lid lag. Another common feature is a smooth eyelid surface with a poorly formed upper eyelid crease.